BEST CARDIAC SURGERY
Devoted to
CARDIO THORACIC AND VASCULAR SURGERY
by
Dr AVINASH DAL
Medicover Hospital
7-1-21, Railway Station Rd, opp. Metro Station Begumpet, Uma Nagar, Begumpet,
Hyderabad, Telangana 500016
India
ph: +91 9848025467
bestcard
- Home

- Coronary Artery Bypass
- Minimal Access Cardiac Surgery
- Valve Repair & Replacement
- VATS & Thoracic Surgery
- Vascular Surgery
- VENOUS SURGERY
- Congenital Heart Disease
- Robotic Cardiac Surgery
- INTENSIVE CARE IN CVTS
- Social Responsibility in Medical Practice
- GUIDELINES
- Articles
- Recent Advances
- Preventive Cardiology
- ACTIVITIES
- Newsmakers page
- Ideas, News and Links
- Dr Avinash Dal
- The Team
- Awards
- Contact Us
VATS [THORACOSCOPY] & GENERAL THORACIC SURGERY
Thoracoscopy started many years back and has been very successful in management of patients with various thoracic diseases and who require surgery. The modality improves exposure as well as reduces the morbidity of long and painful incisions that accompany conventional thoracic surgery. With the advent of staplers and devices such as harmonic scalpel the range of thoracoscopy is increased to even lung resections.
Thoracoscopy is a wide field of procedures that range from diagnostic one's to very serious lung reconstructions. Usually diagnostic thoracoscopies and those that include the basic procedures such as pleural biopsies, drainage of the pleural fluid with biopsy and pleurodesis for recurrent pneumothorax or recurrent effusions can be done by pulmonologist as it is also the spectrum of "medical thoracoscopy". This does not necessarily need a thoracic surgeon.
There are instances where you cannot do but without a thoracicsurgeon such as wedge biopsy of lung, lung resections for various causes, mediastinal node biopsy and mediastinal procedures, removal of tumours from the chest and thymus gland, cervical sympathectomy for hyperhydrosis of the hands. In all these procedures there may be the danger of lung leak or bleeding and both these may cause a lot of risk to the patient hence it is left to the surgeons to do it.
Thoracocopy has a lot of advantages in the form of lesser bleeding, lesser pain and early recovery and maintainance of the lung function. There are reports of better immunological response with these procedures rather than open surgery.

There may be some limitations of thoracoscopy especially if there are dense pleural adhesions and if the patient is not able to sustain a single lung ventilation. In such cases or if there is some bleeding, one may have to revert to open surgery. However, this is not common.
INTERESTING CASES
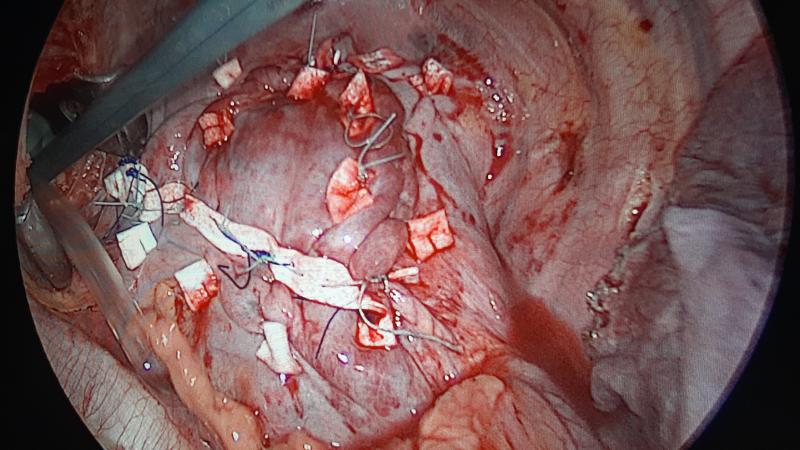
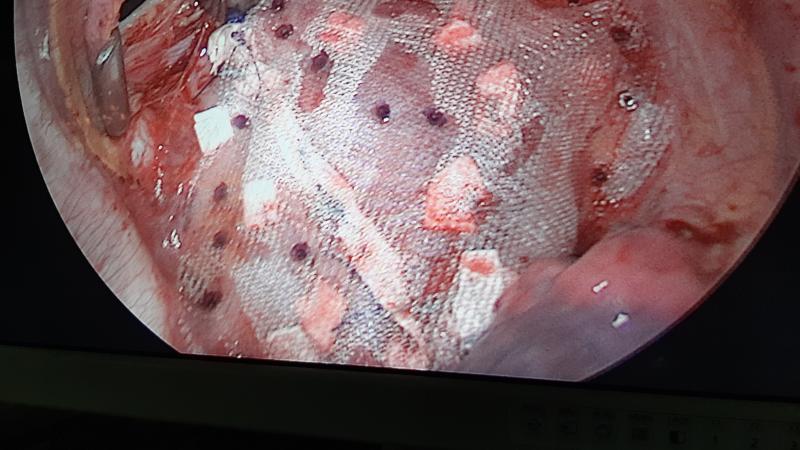
EVENTRATION OF DIAPHRAGM : TOTALLY ENDOSCOPIC TREATMENT
Eventration of diaphragm may be treated by open thoracotomy, laparatomy or laparaoscopy. We had a case successfully treated purely by thoracoscopy [VATS] with plication followed by prolene mesh augmentation. Below are the pre- and post- operative xrays,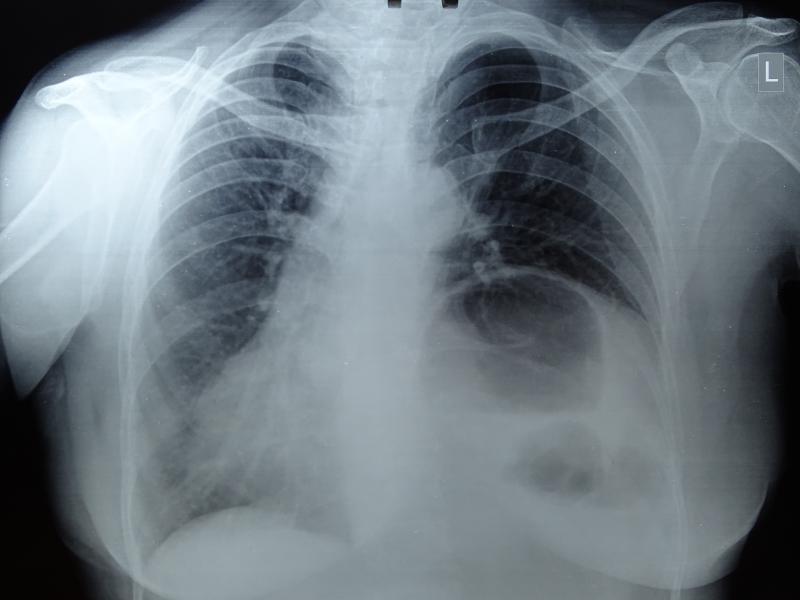
Postoperative xray:

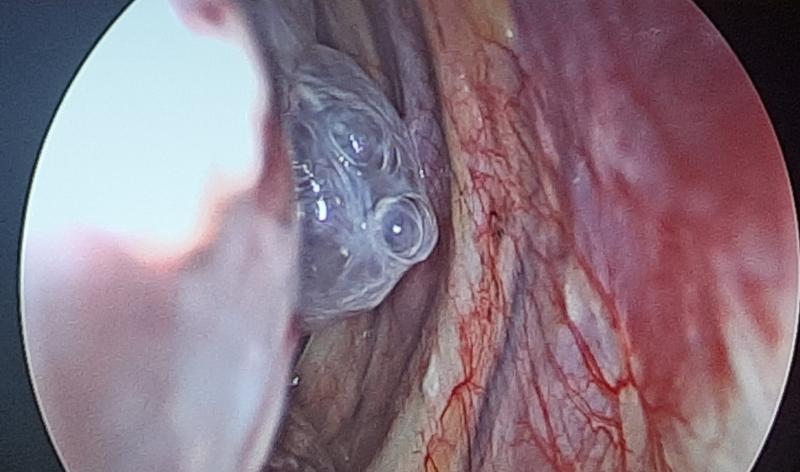
VATS BRONCHOGENIC CYST
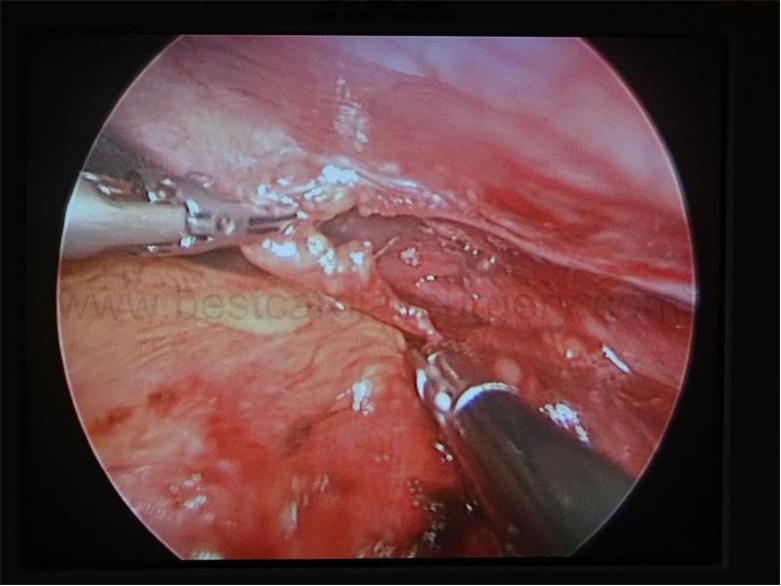
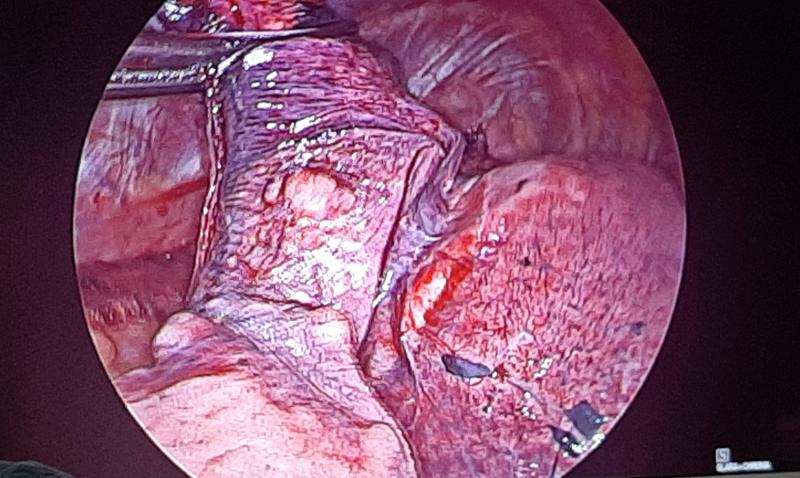
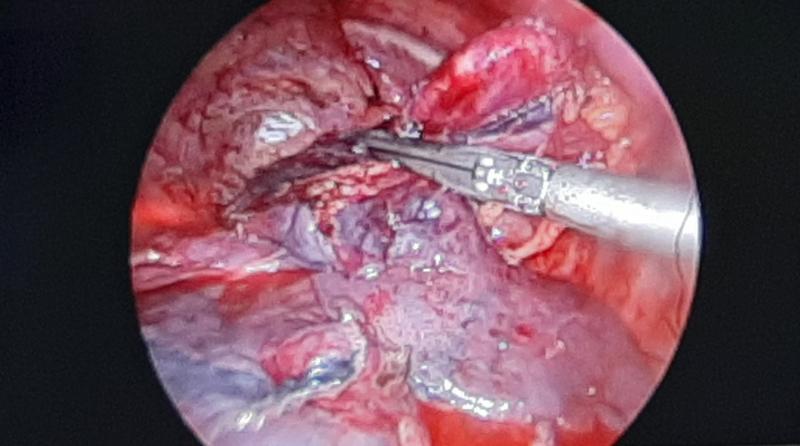
VATS THYMECTOMY
Thymus gland being dissected thoracoscopically by Dr Avinash Dal
Final incisions [after removal of mass]

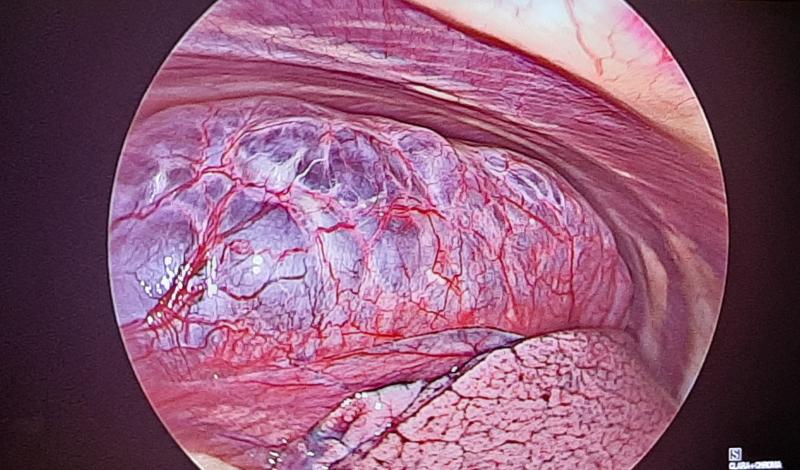
VATS BULLECTOMY
See the large Bulla in the lung even after collapsing the lung
Paper thin bulla of lung: may rupture on the next cough (see below)
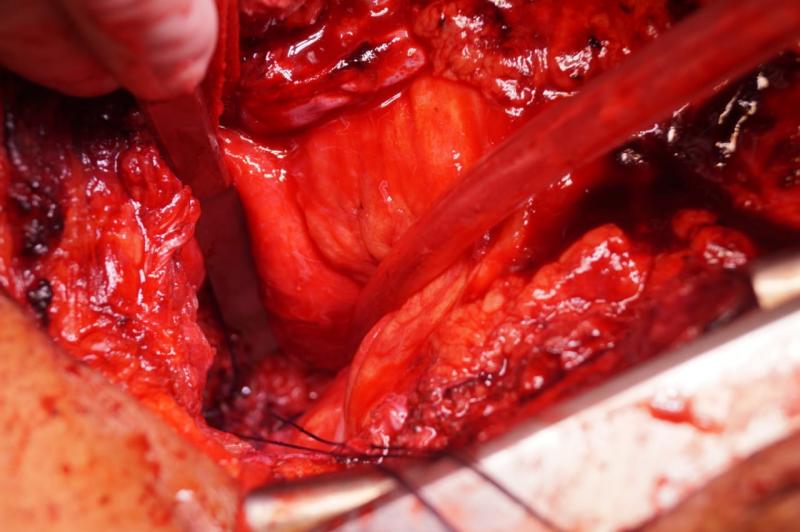
VATS is video assisted thoracic surgery as nowadays no one uses old scopes by looking into the eyepiece.

Besides stapler techniques, one may also suture the lung or any tissue with minimal access or thoracoscopic needle drivers and holders as shown above.
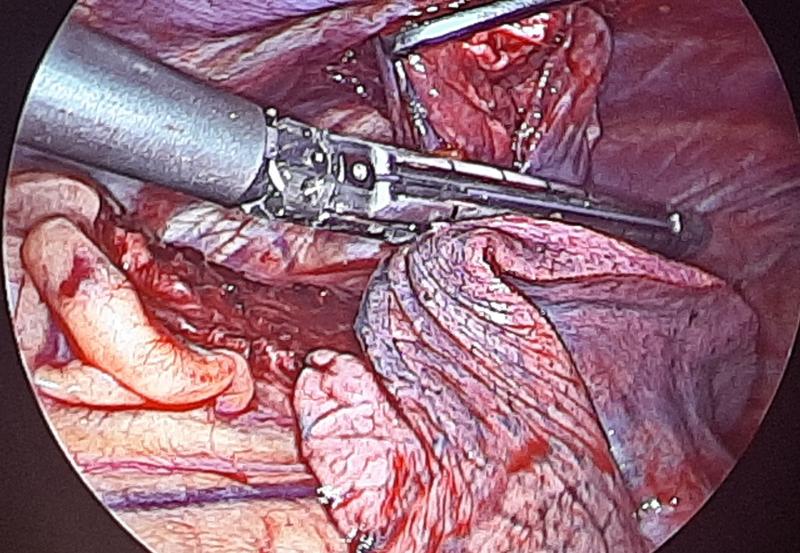
VATS removal of chest wall mass

With miniimal incisions to access inside the chest, there is early recovery and less postoperative pain. Also it has been proved that thoracoscopic surgery has a beneficial effect on WBC activation when compared with routine open thoracic surgery. For the surgeon, the magnification with the scope is great and enhances accuracy

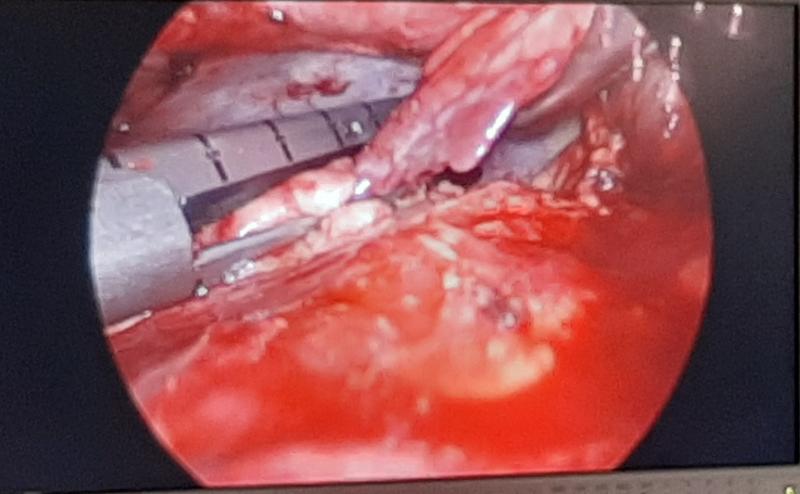
Staple application on lung
 Lung staple-cut with endo-staplers
Lung staple-cut with endo-staplers
TRANS-STERNAL TRANS-PERICARDIAL BRONCHOPLEURAL FISTULA CLOSURE
After 12 years of suffering with a chest tube for persitent bronchopleural fistula, a 55 year old person finally was able to get respite by transsternal- transpericardial bronchial staple ligation and modified Alexander thoracoplasty

above is the preoperative xray showing the residual pleural space and Intercostal tube. Below is the xray showing obliteration and thoracoplasty

Many procedures such as pleurodesis for the recurrent spontaneous pneumothorax and formation of pleuropericardial window for recurrent pericardial collections can be performed besides routine lung and wedge resections and biopsies.
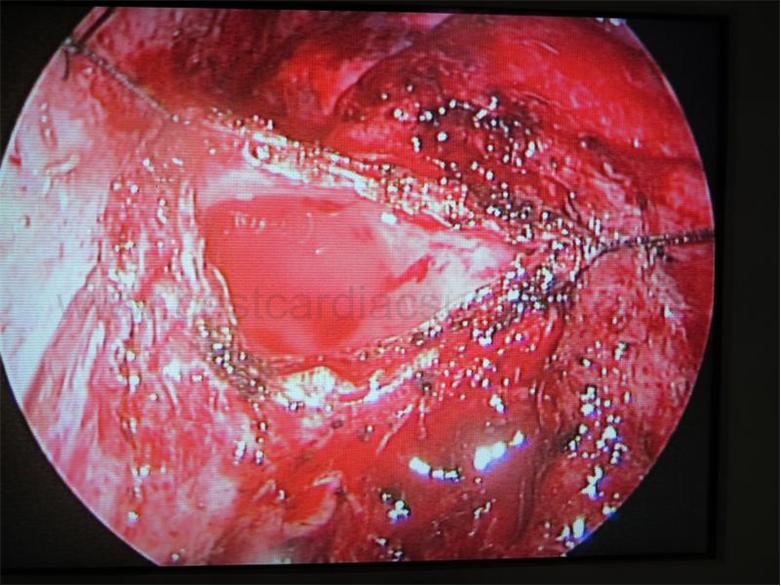
Pleurodesis especially gives excellent results as shown below. One may use abrasion with a gauze piece or even cauterisation of parietal pleura

Final effect of punctate marks on the parietal pleura
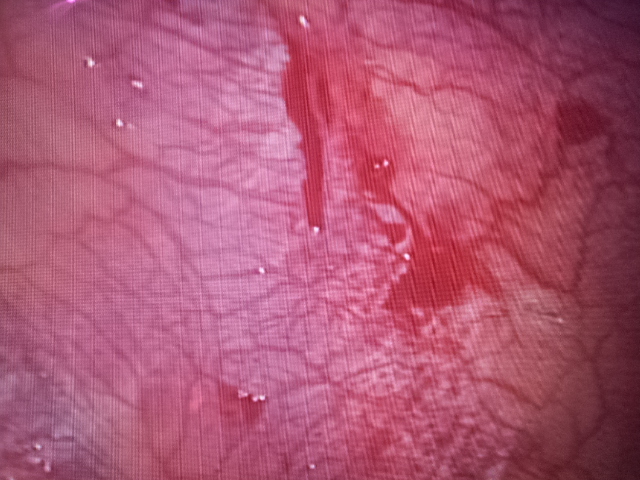
Cauterisation of the parietal pleura gives good long term results. The cauterisation must be done on the rib and not in the intercostal space or else there may be severe neuropathic pain postoperatively
SUBXIPHOID VATS
Subxiphoid approach to thoracoscopy is a new and novel approach that is especially very good for bilateral lung lesions to be operated in the same sitting. One patient had bilateral bronchiectasis and hemoptysis. Bronchoscopy could not ascertain the side of the hemoptysis in the quiescent phase, hence it was decided that bilateral lung resection should be performed.
We performed this through the subxiphoid incision with sternal retraction along with extra port for triangular manipulation. Right middle lobectomy as well as left lingular lobectomy was performed in the same sitting.


 Above Right middle lobectomy via subxiphoid VATS
Above Right middle lobectomy via subxiphoid VATS
Below: Lingular lobectomy via subxiphoid VATS
Medicover Hospital
7-1-21, Railway Station Rd, opp. Metro Station Begumpet, Uma Nagar, Begumpet,
Hyderabad, Telangana 500016
India
ph: +91 9848025467
bestcard